Risk-Based Screening
Screening schedules adapt to age, family history, comorbidities, lifestyle, social risk, and emerging biomarkers.
Front Door of Precision Health
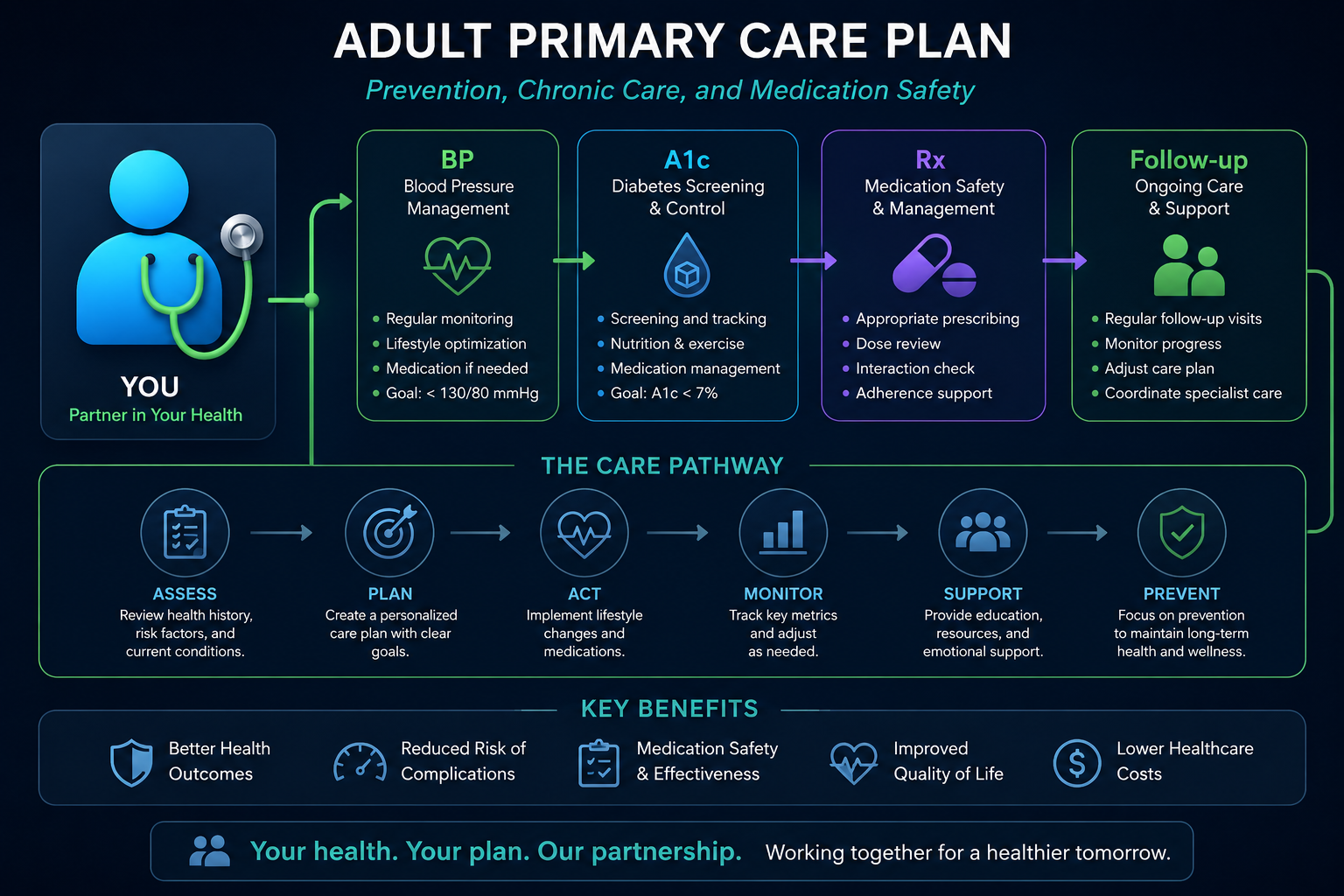
Comprehensive adult care that integrates prevention, diagnostics, chronic disease management, medication safety, behavioral health, and specialist coordination into one longitudinal clinical home.

Abstract
Internal medicine connects prevention, diagnosis, treatment, and follow-up across the adult lifespan. In a precision health model, primary care becomes the coordination layer where genomic risk, laboratory trends, medication history, social context, and patient goals are translated into practical clinical decisions.
Screening schedules adapt to age, family history, comorbidities, lifestyle, social risk, and emerging biomarkers.
Hypertension, diabetes, kidney disease, obesity, COPD, and cardiovascular risk are managed through coordinated care plans.
Primary care aligns specialists, medications, referrals, diagnostic results, patient preferences, and follow-up tasks.
Parts I-II
Internal medicine synthesizes symptoms, physical examination, laboratory findings, imaging, medication exposure, behavioral context, and disease risk into a practical adult care plan.
Vaccines, cancer screening, cardiovascular prevention, metabolic assessment, and lifestyle counseling reduce future disease burden.
New symptoms are evaluated through clinical reasoning, targeted testing, and careful follow-up when uncertainty remains.
Multiple chronic conditions are prioritized by urgency, risk, function, quality of life, and patient goals.
Part III
Primary care turns risk signals into prevention plans that are timely, personal, and realistic.
Blood pressure, lipids, glucose, weight, kidney markers, family history, and lifestyle patterns guide prevention intensity.
Screening for colorectal, breast, cervical, prostate, lung, and skin cancers can be aligned with individual risk and guidelines.
Vaccination plans account for age, immune status, chronic disease, travel, occupational risk, and prior immunization history.
Sleep, nutrition, exercise, tobacco cessation, alcohol moderation, stress care, and social connection are treated as clinical priorities.
Part IV
Internal medicine helps patients navigate overlapping chronic conditions through practical, monitored, and coordinated plans.
Blood pressure care combines accurate measurement, lifestyle support, medication selection, home monitoring, and cardiovascular risk reduction.
Diabetes care integrates glucose patterns, kidney and heart protection, medication safety, nutrition, activity, and patient-centered goals.
Primary care detects and slows kidney disease while coordinating nephrology referral when risk increases.
Respiratory pathways combine diagnosis confirmation, inhaler technique, trigger control, exacerbation prevention, and vaccination.
Older adult care prioritizes function, cognition, fall prevention, medication simplification, goals of care, and caregiver support.
Part V
Primary care evaluates ambiguous symptoms, prioritizes urgency, and follows diagnostic uncertainty over time.
Chest pain, dyspnea, abdominal pain, fatigue, headache, dizziness, and weight change require risk-aware triage.
Testing is chosen to answer specific clinical questions while avoiding cascades from low-value studies.
Abnormal results, pending referrals, repeat imaging, and unresolved symptoms are tracked until closed.
Decision support can surface risk patterns, guideline reminders, drug interactions, and missed follow-up tasks.
Part VI
Precision primary care brings together the biological, clinical, behavioral, and social dimensions of adult health.
Part VII
Primary care must balance access, continuity, complexity, data overload, and equity.
Records across hospitals, specialists, pharmacies, labs, and patient devices can remain disconnected.
Complex visits often require prevention, chronic care, acute symptoms, and documentation in limited time.
Workforce shortages, cost, transportation, broadband, and insurance issues can limit timely care.
Polypharmacy, drug interactions, adherence barriers, and changing kidney function require repeated review.
Early disease often presents with nonspecific symptoms that require follow-up and careful safety-netting.
Care plans must address language, culture, health literacy, bias, and historical barriers to care.
Part VIII
The future of internal medicine is continuous, team-based, data-informed, and prevention-centered.
Risk models can identify patients needing outreach before emergency visits, complications, or disease progression.
Remote monitoring, secure messaging, virtual visits, and asynchronous review can improve access and continuity.
Genomics, biomarkers, family history, and lifestyle data can refine screening and prevention intensity.
Pharmacists, nurses, behavioral health clinicians, and care managers extend primary care capacity.
AI may reduce clerical burden by drafting notes, visit summaries, orders, and follow-up plans for clinician review.
References
Agency for Healthcare Research and Quality. (2025). Patient-Centered Medical Home and Care Coordination Resources.
American College of Physicians. (2025). Internal Medicine and Adult Primary Care Practice Resources.
Centers for Disease Control and Prevention. (2025). Chronic Disease Prevention and Health Promotion.
U.S. Preventive Services Task Force. (2025). Recommendations for Preventive Services.
National Academies of Sciences, Engineering, and Medicine. (2021). Implementing High-Quality Primary Care.
World Health Organization. (2025). Primary Health Care.
Topol, E. (2019). High-Performance Medicine: The Convergence of Human and Artificial Intelligence. Nature Medicine, 25(1), 44-56.
Ginsburg, G. S., & Phillips, K. A. (2018). Precision Medicine: From Science to Value. Health Affairs, 37(5), 694-701.
FAQ
Practical answers about internal medicine, prevention, chronic disease, coordination, and precision health.
Internal medicine translates advanced diagnostics and specialty recommendations into a complete adult care plan that fits the patient's conditions, medications, goals, risks, and everyday life.
Primary care monitors trends, adjusts treatment, coordinates specialists, addresses medication safety, supports behavior change, and follows complications over time.
AI can support risk stratification, guideline reminders, abnormal result tracking, medication safety checks, documentation, triage, and population health outreach while preserving clinician oversight.
Medication reconciliation reduces duplications, interactions, dosing errors, side effects, affordability problems, and avoidable complications, especially for patients with multiple conditions.
Patient-centered primary care combines evidence, clinical judgment, patient preferences, cultural context, access barriers, and shared decision-making into a care plan the patient can actually follow.